
The paper attempts to offer a method to consistently monitor and capture a data eco-system in the everyday of a patient-caregiver relationship. We offer an account of the capture and intermeshing of different types and quality of data sources and their gainful deflection into a methodological protocol for ethnographic engagements. We call this the ‘360° feedback’ ethnography and elaborate its underlying methodological process in this paper. Building on the live feedback obtained from various stakeholder activities in a care ecosystem, we propose how a 360° feedback can enrich regenerative knowledge.
INTRODUCTION
The art and praxis of care management is a contextually embedded one; not only is it reliant on the nature of the care giver-patient relationship but also the coming together of a tethered eco-system of location, information and infrastructure. While penetration of the internet of things is providing opportunities for creating tools to diagnose patient conditions and care plan interventions, caregiving offers specific challenges related to the situational and the emotional hubris surrounding the roles and relations between caregivers and the patient who are united by more than the bond of caregiving. Alongside the emotional and exhausting interpersonal exchanges that happen in caregiving scenarios, multiple caregivers, including non-professional, informal and familial caregivers are needed to loop the eco-system of care management. The use of pervasive computing for perpetual and assured gathering of patient data presents an opportunity to not only have deeper understanding of patient’s condition but also to engage various stakeholders in caregiving ecosystems; perhaps to even engender patient-centric technologies with humane overtones.
This paper will offer an instantiation of how ethnographic methods have approached big data – by big data we mean various types of quantifiable data in a caregiving situation encompassing key persons, stakeholders, caregiving practices and contextual contingencies. Making a case for big data and ethnography as a relationship in generating interpretative insights based on human behaviors [what Curran [2013] references as ‘Big Ethnographic Data’] we dwell on a research contribution towards transforming consumer centric healthcare services. In the attempt to offer a method to consistently monitor and capture a data eco-system in the everyday of a patient-caregiver relationship, we offer an account of the capture and intermeshing of different types and quality of data sources and their gainful deflection into a methodological protocol for ethnographic engagements. We call this the ‘360° feedback’ ethnography and elaborate its underlying methodological process in this paper. In a sense this paper is less about the ethnography and more about an approach assimilating the sensibilities of big data and ‘thick data’.
Previous research (Fiore-silfvast and Neff 2013) talks about data valences in digital health data ecosystems, and comments about the relevancy of data in social, organizational and institutional scenarios. Even if patient mediated or pervasively captured patient-end health data, such as the one proposed by Human API (Baek et.al. 2013), are obtained simultaneously, the impact of invisible work (Unruh and Pratt 2008) and the caregiver’s participation (Corbin and Strauss 1985) in chronic disease management remains, well, invisible! Perhaps the live nature of every care activity can provide a 360° knowledge of care delivery and further improve care interventions [Interestingly, in the domain of customer experience consulting, ethnographers (Slobin and Cherkasky 2010) have emphasized data acquisition to gathering customers’ experiential understanding. They call this “360 view of my customer”]. Given the diverse profiles of caregivers, multitudes of processes and information exchanges, and the longitudinal nature of chronic disease progression, having a 360° view of the care ecosystem becomes even more important.
An ethnographic study with 22 patients from 18 families in three tier-two [ cities with under a million population] in India foregrounded the study to capture the eco-system of care management knowledge – the latter included a plethora of players and their relationship to care management. We chose smaller cities where care giving is more familial and not outsourced to a hospital [ more common in the big metropolises of India due to better hospital infrastructure ]but nonetheless intersect with professional caregiving practices. It gave us a snapshot of the dynamic challenges faced by caregivers within a family and a window to think about opportunistic technology interventions. Our initial assumption centred around non-adherence to medication, unobserved disease symptoms and missing information requiring continuous involvement, attention, and coordinated dialogue exchanges among and between the diverse sets of patient – caregiver duos. Moreover, whether remote or situated, caregiving is mediated through psychic-emotional closeness between the caregiver and patient with consequences for care outcomes. There is a critical need for building communication strategies catering to a caregiver’s involvement in the care process, integrating their knowledge and experience in a specific patient monitoring ecosystem. We address this gap capturing patient and caregiver knowledge into a caregiving ontology (CO).1 The knowledge categories we generated about caregiving protocols and ensuing relationships are directly informed by our ethnographic observations of caregiving in the Indian family.
Ethnographic vignettes gathered from homes and contextual scenarios presented motley arrangements of between caregiver-patient relationship dynamics. We explain these scenarios through a trust-persuasion relationship quadrant, representing the different scenarios and extent of trust and persuasive strategies among patient and caregivers depending on care availability and the nature of caregiver-patient kinship /social ties. We further substantiate our findings via a technology probe called iSwear including the patient-caregiver communication repertory, a feedback mechanism about the patient’s everyday care regime, patient information about physical activity and adherence or the lack of it to everyday medicine in-take and consequent changes in communication patterns caused to regular patient – caretaker communication behaviours. We created knowledge categories of care [we also call it care ontology, CO]that considers, not just the patient’s clinical and activity data but the collaborative nature of caregiving, multiple care communication protocols entailing accurate and generative knowledge of a care ecosystem. The knowledge categories or CO, are built from accounts of patient data which are periodic [sometimes self-recorded or fetched from the wearable we designed], and caregiver data such as situated availability, knowledge and extent of participation in care. Contextual interviews during the iSwear pilot study and logs fetched from iSwear helped us to map caregiver profiles based on care contribution and patient-caregiver trust levels. While Caregiver profiles and their relationship to the patient were vital , capturing right amounts of patient care feedback data, at critical moments of caregiving helped to comprehend not only a specific care ecosystem but to evolveg a generalizable and ontological understanding of communication practices in the patient-caregiver everyday repertory. And, we call this ‘a ‘360° Feedback’ ethnography of chronic Care knowledge generation’.
This paper is arranged to reflect the primacy of the ethnographic process in framing caregiving praxis and knowledge categories of care management. We begin with an in-situ understanding of familial care giving segueing into design implications and the actual building of the wearable iSwear aiding communication protocols of chronic care management. We then elaborate the generation of a care ontology/CO, focussed on the centrality of the caregiver’s relationship to the patient, routines/praxis of caregiving and types of everyday communication protocols between the care giver and patient. We reiterate that this paper is as much a piece on the ethnographic method as it is an approach to synthesise ethnographic insights with the generation of a data eco-system.
OVERVIEW
Over the last decade studies have emerged around social, economic, and health concerns of general ageing (Vines et.al. 2015) and chronic diseases in particular (Wanger et.al. 1999). Patient compliance in health care is one of the significant factors under research scrutiny. We begin the literature review with an overview of Chronic Disease Management (CDM) and the role of caregiver in care delivery. We move on to the social and structural context in the family caregiving scenario in order to understand the relationship dynamics in caregiving, role-playing, construction of trust and their effects on patient motivation and emotional support. Finally, we look at how technologies have evolved to assist chronic disease management, and how this data could benefit care interventions.
Caregiving and Chronic Disease Management
The caregiver’s role has been widely discussed in HCI literature (Vines et.al. 2015). We took inspiration in the work of Corbin and Strauss (Corbin and Strauss 1985) who speak of trajectory work, which explains the nature and complexities of care work required during acute health conditions and general chronic problems. Higher trajectory work requires additional experience and professional training in caregiving while lower trajectory work can be done at home. A lot of the work that informal care givers (i.e. family members) do is low trajectory work like scheduling appointments, managing prescription and transportation issues. Corbin et al. mention three lines of work in CDM, in the case of home-based caregiving, care givers perform trajectory work such as monitoring patients, recording temperature, checking medication doses, etc. It emphasizes the semi-professional character of the work of informal caregivers as these also included activities such as fostering a sense of independence in patients while simultaneously enabling, motivating and persuading patients to follow prescription etc. The caregiver’s ability to perform medium and higher trajectory work (if required), is largely dependent on her experience of performing low trajectory work and an understanding of the patient’s condition. Caregivers are heavily involved in day-to-day quotidian activities related to chronic illness management along with providing emotional work having a significant impact on a caregiver’s lifestyle (Chen et.al. 2013). Thus, we consider the interactive behaviors and exchanges of dialogues between a caregiver and a patient, especially in the emotionally loaded setting of a family, as a crucial factor in influencing a caregiving scenario. These, we believe, were constitutive of persuading and motivating the patient to positively respond and comply with caregiving activity. Our ethnography also focused on understanding the caregiver’s nature of needs and preferences in managing their kin’s health and the accompanying challenges to these activates.
Social Structure of Care
We begin by looking at the three main aspects of the structure of care giving. These are; one, the role of formal caregivers who may not be family members; two, informal caregivers, who are family members; three the immediate social support such as friends and persons from the neighborhood supporting caregiving as activity. We took inspiration from the line of work typology by Strauss, but while arriving at the three main aspects we specifically focused on the patient-caregiver relationship. Much of caregiver literature clearly also draws a distinction between physical or practical support (Gandhi and Bowers 2008) (i.e. in case of formal caregiving), and emotional support (Young et.al. 2004) (i.e. in case of informal caregiving). The role of familial caregivers, particularly spouses, children and siblings, as the primary providers of emotional support (Keating et.al. 2003) have been shown as playing an important role in persuading a healthy lifestyle and promoting wellness (Parker et.al. 2012) in patients. Additionally, patients also receive care from relatives who are not living with them (i.e. remote caregiving scenario). Literature suggests that care received in the case of the remote scenario is more likely to be functional than emotional (Allen et.al. 1992). These studies underline the fact that it is moot to generalize the type and extent of caregiving provided by family members and immediate social surroundings.
Furthermore, formal caregiving is largely restricted to hospitals, and family caregivers do most of the care arrangements at home (Dolenal et.al. 2002). Studies show that caregiver stress is reported to be associated with variables such as family income, age of caregiver, kinship relationship, caregiver’s attitude and certain attributes of the care recipient (Jamuna 1997). Apparently, the way a child manages care for a parent might be very different from a spouse managing care for her partner. Thus, we draw our focus on understanding different roles that caregivers play in a family caregiving setting and how the relationship does influence patient wellness and adherence to medication. We further emphasize understanding the differences between the contexts of filial versus conjugal caregiving. To the best of our knowledge, there is no study that illustrates the differences in caregiving behavior among different familial roles. Furthermore, there is a need for understanding multiple types of persuasion and motivating behavioral strategies in a family caregiving setting.
Technology and Chronic Disease Management
Design for Chronic Disease Management (CDM) and Patient Monitoring have been widely discussed in both medical science and gerontology. Researchers (Chen et.al. 2013) explain the importance of designing for patient-caregiver integrality, especially due to the burden of care negatively affecting the health and wellness of caregivers, leading to anxiety and stress. Previous work exploring the caregiving process and how technologies can be designed to offer improved physical, social and emotional support to patients considers the collaborative nature of caregiving (Conclove et.al. 2004). Apart from sensing technologies, very little research has focused on facilitating caregivers to effectively persuade patients.
Systems and devices are being developed to enable caregivers to monitor patient activities from distant locations (Duncan et.al. 2009) and to aid a caregiver coordination network (Tang et.al. 2012). Wireless health communication systems and caregiver communication system for home environments provide patients with a direct link to a caregiver. These interventions permit a patient to send a request for assistance directly, and provide for two-way voice communications. Most of the above-mentioned interventions have been designed with a technologically deterministic point of view and overlook the trust and relationship interplay between patient-caregiver communications. Additionally, such systems focus on an acute scenario of caregiving where patients may be bed-ridden. Notification communications are usually designed to target the onset of acute conditions for varied latency of occurrences that may occur abruptly. In case of chronic illness, the onset of a deteriorating condition is generally gradual, often insidious, where technological interventions tend to become indecisive with uncertain diagnosis and prognosis (Holman and Lorig 2002). There is a need for pervasive and continuous patient-caregiver communication support wherein care activity becomes longitudinal and patient motivation is framed by the caregiver’s effective persuasion.
To the best of our knowledge, to date there is no study examining the usability and perceived usefulness of such systems. More importantly, most extant studies talk about usability and adaption, but none focus on the multi-user aspect (where you have a patient as the primary user and a caregiver as the secondary user of the system).
METHODOLOGY
We conducted two studies; the first comprised of contextual interviews with 18 care givers and 22 patients in 18 families living in the cities of Bengaluru, Bhubaneswar, and Mumbai; the second a preliminary evaluation and user study with iSwear, our communication and patient mentoring system, in 3 families, 2 in Mumbai and 1 in Bengaluru. Before we move on to describing the social contexts of caregiving in our sample, here are a few broad yet key questions framing our investigation and the more specific investigations of in-situ and personal interviews.
- What is being measured – What is the type and extent of formal support caregivers provide to the patient?
- How is it being measured – What are the present methods of monitoring, information sharing, and information exchange among the patient and caregiver in various contexts of familial caregiving?
- What are the predominant challenges– What are the caregivers ‘every day pain points’ and how do they impact their day-to-day caregiving activities and broader lifestyle?
Sample
The sample consisted of 10 in-person caregivers and eight remote caregivers. Eight out of 18 of the participants (in-person: eight; remote: zero) were either wives taking care of husbands (i.e. six) or vice versa (i.e. two). We will address them as conjugal caregivers in rest of this paper. The rest 10 of the participants (in-person: six remote: four) were children taking care of their parents. We will address them as filial caregivers. In total we had nine female and nine male caregivers.
Our sample had no caregivers falling in the category of conjugal-remote scenario- by remote we mean spouses, still married but living in different homes. The term ‘remote’ is used, for the purposes of this study, to exclusively denote physical distance. We did not have the wherewithal to include emotional distance in our research framework. Moreover, physical distance was one of the implications for design in this study influencing the iSwear system. We also had spouses living together impart remote caregiving to partners during specific hours in a day from their work places during working hours. Instances of caregiving such as being vigilant about food and medicine intake, and follow-ups with formal caregiver would often occur in a remote scenario. Thus we considered data from conjugal-In Person scenarios for analysis, in which the caregiver had been away from the patient for a limited amount of time. We had cases of extended families [with more than two generations of a family lived together where multiple caregivers are involved in providing various degrees of support to the patients. Six were joint families in which caregivers took support from other family members. Extended family members such as in-laws or close relatives take up caregiver roles for a specific duration accompanying the patient for periodic checkups, or other activities when the primary caregiver is not around. Most of the patients from these 18 families have had at least one acute episode during which our participants have managed their care. All the participants were reasonably versed with a few computer/mobile applications and health devices available for patient monitoring and adherence. Two caregivers were also versed with using bedside systems such as a health-buddy, but only in a hospital setting.
Table 1. Preview of selected sample
| Caregiver’s Relationship | Remote | Situated | ||
| Male | Female | Male | Female | |
| Filial (10) | 3 | 1 | 3 | 3 |
| Conjugal (8) | 0 | 0 | 2 | 6 |
All families belonged to the middle-income group in urban India having annual income ranging between USD 3000 and 10,000 with medication alone costing USD 150 to 500 per month for every patient. Additionally they were incurring cost of other expensive medication in case of shoot in problem and regular checkups. They were all taking continuous professional support from established hospitals in their cities, sometimes even further away in bigger hospitals, based on the availability of specialization and expertise. A basic fall alarm, tracker bracelet or bedside alarm that can be used at home would cost anywhere between USD 100-250 but chances of their adoption are extremely low in Indian homes.
Some of our participants had one or more chronic conditions – diabetes, arthritis, hypertension, lung disease, renal disorders, and heart problems. It is important to note that the kind and extent of medication or care required may differ in all of these diseases, but the prescribed self-care behaviors (Shrivastava et.al. 2013) largely remains the same. These self-care behaviors emphasize healthy eating, physical activity, monitoring blood sugar, compliance to medication, problem-solving skills, healthy coping skills and, risk-reduction behavior.
To achieve a more diversified and deeper understanding of the caregiving context we developed an interview question schedule based on our early set of broad research questions to investigate the specifics of care giving in a set of familial social contexts. Two authors of this paper conducted interviews mainly in the home setting of caregiving. Each interview lasted for 60 to 90 minutes. All interviews were recorded and transcribed. The interviews and prototyping iSwear took a duration of 3 months, which was followed by a month of the iSwear pilot study.
Method
We analyzed our notes taken during fieldwork and interview transcripts using an affinity mapping exercise (Kawakita 1991) and evolving design themes clustered according to their similarity, dependence and proximity of relationship. Themes were identified from the body of evidences gathered from the field and used for the ideation of a caregiver assistive system or tool. Some of the key themes identified are motivation, persuasion strategies, monitoring and vigilance challenges, information flow, role reversals and conflicts. Patient monitoring and vigilance emerged as a key challenge influencing patient-caregiver relationship as well as caregiving dialogue exchanges, and conflicts. Success of persuasion strategies strongly depended on the effectiveness of monitoring. This motivated the design, implementation and testing of iSwear, a wearable device for patients with chronic illness, which can send messages to caregivers about patient activity related to food & medicine intake. An initial exploratory evaluation was conducted with 3 families, where iSwear was given to these patients for a week. We monitored usage patterns through patient-caregiver sms/call logs and followed up with in-person interviews in the homes of the families. We faced limitations in time to extend our probes during the pilot but the period afforded an intimate view of caregiving routines that formed around the technology probe and the challenges thwarting a more successful adoption of technologies for caregiving. We discuss the findings from our ethnography in detail in the next section.
Design of iSwear
This section will explain the design of the CDM communication and monitoring system ‘iSwear’. primarily informed by the ethnographic insights derived from caregiving situations.
iSwear is a system focalizing caregiving as a set of key practices in persuasive heath care delivery in family settings. Our aim was not to build a prototype with full capability and accuracy, but to look at usability and acceptance of such a system in a familial caregiving scenario. Our ethnography of familial caregiving revealed caregiver-devised patient monitoring and vigilance strategies focused unduly on the need for assurance and pervasive communication with the patient. With iSwear we aimed to aid some of these strategies while placing the caregiver as the central actor in caregiver-patient communication practices.
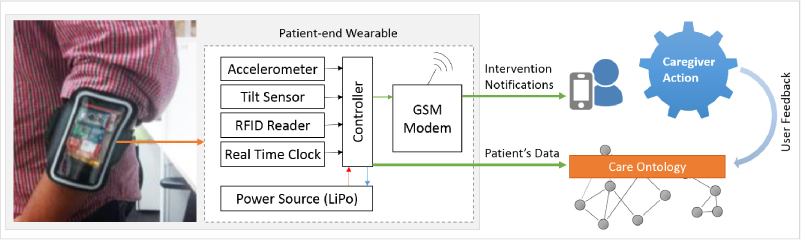
Figure 1. iSwear device & its components
We considered measuring physiological parameters such as heart rate, ECG, EEG, activity and food intake, to measure and manage multiple chronic conditions. Considering the focus of our study and caregiver intervention areas, we narrowed it down three parameters. These are 1. Measure of daily physical activity 2. Time of medicine intake 3. Time and portion size of food intake. A wearable system, iSwear, was designed to measure these physiological parameters. Figure 1 shows the complete component diagram of iSwear. iSwear consists of three main sensors, the accelerometer, tilt sensors and an RFID transceiver. These were used to measure the above-mentioned patient activity data. RFID tags placed on the medicine bottle helped to inform about medicine intake. The data collected from the sensors of the iSwear is converted into meaningful information about patient activity with the combination of different data streams.
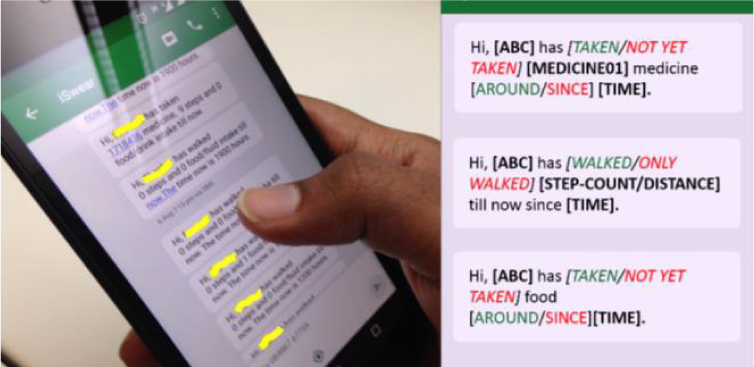
Figure 2. Message variations received at Caregiver’s Phone
The GSM module attached to the device consisted of a specialized modem with SIM card, for sending SMS to the caregiver at a frequency of four times a day (i.e. 9am, 12pm, 3pm and 6pm). Figure 2 shows different variations of the SMS designed for actions of medicine intake, walking, and food intake respectively.
Design of Caregiving Ontology – Caregiver as Agent
To capture caregiver activity or responses on the received system messages, a caregiving ontology(CO)was designed. We use the standard OLW (Web Ontology Language) to create entities- in our case, caregiver data about existing caregiver – patient social and kinship profiles and their contextual information (such as experience of caregiving and locational availability) were created as ‘caregiver’ entity to the CO. The system would query the entities and their inter-relationship to trigger notification for any care activity related reporting. Patient entity values were analyzed in runtime, and contextual information about patient activity and medicine adherence were added to the ontology as another set of entities.
Patient-end disease information and contextual information about patient activity and medicine adherence were added to the ontology as object values. Caregiver data about existing caregiver profiles and their contextual information (such as the experience of caregiving and locational availability) are added as ‘caregiver’ entity to the CO. The CO would store all the caregiver responses as an object value for the entity caregiver.
A simple SPARQL (Simple protocol and RDF Query Language) pseudo-code run on the patient entity for the CO is used to understand the required caregiver response, and thereby send an actionable notification to the caregiver. The queried activity is then sent to the different caregivers based on their type using the messaging system.
SELECT ? cgType ? cgFeedback ? cgIntervention ? Recommendation
Where
{
cgIntervention : Activity
cgType : CGc-s
cgFeedback : hasRecieved ? hasResponded ? hasActed ?}
Once the intervention type and the nature of the caregiver have been identified, predefined message templates are used to create recommendations. These recommendations are pushed as notification to the caregivers. The caregiver messaging flow and their responses to these notifications informs us about the real-time human interaction in a caregiving ecosystem. The system places the caregiver as agent in triggering the messaging activity.
EVALUATING THE FEEDBACK DATA ECOSYSTEM
We conducted our preliminary field study with 3 families (2 conjugal, 1 filial, all in-person caregivers). All 3 patients were above 60 years of age and suffering from type-II diabetes mellitus. iSwear was given to the patients who were asked to wear it for a period of one week from 8am to 8pm. This was the time when these caregivers or patients were generally out at their workplaces. We took care to familiarize and orient users to the device and the nature of our experiment. The RFID tag was stuck to the medicine bottle/strip and dosage timing and frequency was noted. The phone number of the caregiver was noted and set as default number to send SMS through iSwear. An SMS & Call Log Backup application [33] was installed in the caregiver’s phone with their consent. We also gained consent for all phone conversations to be time logged and recorded.
We observed wearable notification response and patient action response through phone logs and wearable logs. Wearable notification response would inform us about how caregivers responded to the received notification and in how much time. The patient action response would inform us about the patient activity once the caregiver has responded to a notification in a certain way, such as making call to the patient. Additionally, at the end of every week, both the patient and the caregiver were interviewed for system feedback.
INITIAL FINDINGS
Our findings are focused on understanding care arrangements in Indian families. We probed on the nature, order and extent of various caregiving activities, health record keeping and information management involved in effective care delivery. We took specific care in understanding family dynamics that shaped and hovered around caregiving activity in order to focus on the caregiver-patient interactions and emotions surrounding the act of caregiving. We observed various forms of persuasion and motivation strategies, ranging from the subtle to the distinct, in a caregiver’s repertory of practices for wellness compliance. We probed for the overt and covert needs that caregivers expressed with the current system of access to health monitoring technologies and CDM aids. Location closeness (i.e. remote and in-person caregiving) also provided us insights on different caregiving needs and concerns.
We represent the trust-persuasion quadrants of caregiving scenarios in Figure 4. These are 1. Filial-Remote (FR), 2. Filial-In Person (FI), 3. Conjugal-Remote (CR), and 4. Conjugal-In Person (CI). This representation helps us understand the aspects of trust and persuasion among filial or conjugal caregivers with their kin. The remote and in-person caregiving setting represents the location closeness between caregiver and the patient. While experience represents the number of years spent with the patient as a caregiver, we also found the parameter of experience complimenting the trajectory work representation (Strauss et.al 1985) as caregivers gain in understanding of the patient’s explicit and implicit needs with experience. With gain of experience in longitudinal chronic caregiving, the lower trajectory work becomes part and parcel of a caregiver’s daily lifestyle. However, the same representation may not be true in case of acute episodes, which requires higher trajectory work.
We explain the aspects of trust, persuasion and roles in these quadrants in the following sections. The quadrants themselves are informed by the affinity analysis we undertook to process ethnographic data. We focused on the specifics of the remote and situated care and the emotional and interactional differences among and between filial and conjugal caregivers. These relationships have been mapped in the form of the proposed quadrant.
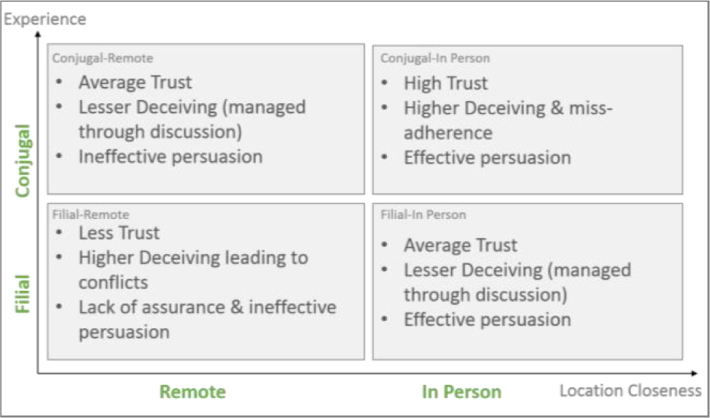
Figure 4. Trust-Persuasion Quadrant in Caregiving Scenarios
Levels of Trust & Assurance in Caregiving
Caregiving goes beyond just physical and practical support as chronic patients seek consistent and continuous emotional support. We found that both filial and conjugal caregivers were involved in providing emotional support along with lower trajectory work [Ref] . It was more evident in case of remote caregiving. One of the caregivers mentioned, “I remember, my sister who is staying in US, was very busy with something and was not responding to her calls. My mother created a Facebook and twitter account all by herself and followed both of us. – (U02/FR)”. Being remote the patient was seeking assurance, and from our understanding every caregiver wanted some kind of assurance consistently about the patient’s well-being. In one case, a conjugal caregiver mentioned, “We take all kinds of precautions. But biggest challenge in monitoring is to know, if we are doing enough and we are going good. – (U15/CI).” This was her major pain point. Perhaps seeking assurance is mutual.
In the case of filial caregiving a common question that every caregiver is concerned with is, “are we doing enough”. Filial caregivers seem to need assurance on their caregiving performance with an over-emphasis on the patient’s speedy recovery. In one instance a caregiver mentioned, “She [mother] first says whether she is doing good or not, I feel that is kind of very minimal information. We need to do something more. – (U03/FR)”. This particular case was a remote caregiver with less awareness about the patient’s adherence to medication. In another case a filial in-person caregiver mentioned, “for an emergency we are given a common number but not the doctor’s personal number. For some case I would want to know if I did anything wrong – (U06/FI)”. He wanted to remain assured in this case with the doctor’s personal number. This indicates how filial caregivers continuously seek professional support and are open to discuss their shortcomings.
Caregivers both filial and conjugal are aware of the patient’s getting around health and medication routines, sometimes even lying about their medical compliance. Caregivers ensure they have complete knowledge about the patient’s condition and doctor’s prescriptions and recommendations. In one instance a conjugal caregiver had her house help accompany her husband for a regular health checkup session. She insisted to know what the doctor had mentioned about her husband’s condition in detail. We found more examples of vigilant arrangements in the case of filial caregiving scenarios. In one instance an FR caregiver was doubtful whether his parents were taking enough care, and thought her remoteness was a limitation. She mentioned, “Not really, I thought that they are taking care of themselves. They have also told me that, but I do not know what is going on behind the scenes. – (U02/FR)”. Many filial caregivers mentioned about the need of continuous monitoring. Such as, “Other than walking and physical activities, food is a big change. But right now we don’t have any means to monitor. – (U12/FR) “. Apparently an in-person filial caregiver confronted his father for smoking under cover. We found multiple such anecdotes of conflict in the case of filial caregiving. This indicates less trust and a stressed exchange in the filial care-giving situation.
Higher levels of patient-caregiver trust were found in apparently all the cases of conjugal caregivers. It is often due to the lack of surveillance/supervision in care or vigilance arrangements that leads to the patient’s non-adherence. We observed a caregiver often times is aware of the workarounds patients indulge in. A caregiver mentioned, “I know he goes out and eats Samosas (fried snack). At least he is not hiding that from me. – (U15/CI)”. This acceptance revisits the aspect of experience in work trajectory theory. With experience the lower trajectory work becomes a part and parcel of caregivers’ lifestyles. It’s the specific or elaborate care activity or higher trajectory work (such as a newly prescribed injection) which are performed with a conscious effort.
However, the same is not true in the case of a filial caregiving scenario. In almost all the cases we found filial caregivers to be very particular and vigilant about patient adherence to prescribed heath procedures. A caregiver mentioned, “I accompany papa all the time, whenever he goes out to the neighborhood market. – (U06/FI)”. Filial caregivers go that extra mile, being conscious to gain caregiving experience. This points to filial caregivers seeking higher assurance on caregiving performance as compared to conjugal caregivers. To cite an extreme case, a remote caregiver moved back to live with his parents: “I was constantly worrying about getting reassured… about their [parents] medical habits and compliance…”
Both patients and caregivers want assurance in whatever ways, small or elaborate, about each other’s whereabouts and are seeking to integrate them into their everyday rhythms and practices. But filial and particularly remote caregivers externalized it as a pain point. Both filial and conjugal caregivers deal with it through specific strategies, such as checking the pill inventory or tracker, getting vigilant help from neighbors or the house help. Conjugal caregivers, on the other hand, with higher levels of trust, often confront loopholes in vigilance arrangements or non-adherence by patients. In cases of filial care giving, similar situations lead to situations of conflict and resistance with the patient.
Contextualizing Motivation & Persuasion for Perpetual Care and Assurance
The art of persuasion in care management is an immersive and embedded contextual phenomenon; not only is it reliant on the caregiver-patient relationship but in multiple relationships within the eco-system of care. A powerful example is one we derived from insights studying contextual cues and the consequent strategies caregivers use to gain trust and thereby persuade the patient to adopt care. Caregivers make that extra effort to motivate the patient to adhere to the wellness regimen. We found filial caregivers applying different strategies to persuade the patient. Such as, “Making sure that harmonium [an accordion based organ commonly used in India] is accessible to her. She could sit and practice it, on musical scales. So trying to distract her from her illness. – (U04/FI)”. In another instance, one filial caregiver used to take her mother to a particular vegetable store so that she would walk that extra distance daily. Interestingly a filial caregiver had placed a measuring cup at home so that the renal disorder patient would have a better understanding of the quantity of the water intake. The caregiver placed the measuring cup at strategic locations at home and always added ice to water for a feeling of drinking more water than what was consumed.
Role Playing and Role Reversals
The roles and the ensuing dynamic between caregivers in the course of care practices, the nature of trust built in the course of caregiving, and evolution of persuasive practices to comply with CDM/healthcare by the patient are vital to understand for designers and technologists.
We observed that in filial caregiving, parents found it challenging to accept their children as caregiver. In many cases these role reversals are gradual. But in cases of an acute episode and the chronic condition thereafter, such role reversals often happen suddenly and the relationships remains never like before. The sudden change of roles brings about defiance in accepting care from children. We found multiple anecdotes of deceiving about medicine and health checkup activities during our interviews. These lead to arguments and conflicts between caregiver and the patient. Moreover constant nudging activity from filial caregivers led to patient self-reliance issues. A filial caregiver mentioned, “She [patient] has been a caregiver for everybody and now the roles are being exchanged. I hope it doesn’t reaches to a point where I have to do something more than what I am doing right now. – (U04/FI)”. In another instance another filial caregiver mentioned, “They [parents] didn’t want to bother me, that’s what they are thinking. They are thinking that I am having a good life, studying. They think that I should not be bothered with all these things. – (U10/FR)”. This indicates something more than just an issue of role reversal. It was observed that patients suffer from a loss of self-reliance and often consider themselves to be a burden for their children who are now the caregivers. Thus, they often mask or become deceptive about their condition. Role reversals were specific to the filial arrangements of care giving, possibly arising from the parenting culture and age-specific cultural protocols in Indian communities. This makes for a fascinating future research proposal in the domain of familial health care practices.
FINDINGS WITH THE ISWEAR DATA ECOSYSTEM
Initially we faced challenges to recruit families with filial or conjugal caregivers for their kin suffering from chronic illness, and who could be monitored consistently for the running time of the study. iSwear brought a determinant shift in caregiving activity and dialogues of persuasion. All three families acknowledged the usefulness of such a system but duration of one week was not enough to illustrate and quantify the desired outcome. Product design and usability of the wearable was also a limiting factor to adoption but we had valuable inputs on the effectiveness of communication and reporting protocols during this study. We present some of the initial observations in the following section.
iSwear was originally sending messages only to the caregivers. All three users, who are patients in the familial caregiving relationship, suggested that they also receive the message being sent to caregivers. [There was a feedback mechanism in the form of a beep when an SMS was sent from iSwear to the caregiver who was remote at that time] The wearers of iSwear, wanted to make sure that the correct information was being sent to caregivers. Apparently they indicated towards the absence of any engagement in wearing the device. A patient asked, “How would I know if the sms is not annoying my wife? Can I do something about it? – (CI)”. Both conjugal partners were seeking parity and transparency in communication. Retaining the patient’s independence and a sense of comfort while being monitored regularly came out as an important concern. A patient mentioned, “Why sms her (caregiver) all the small things”.
Patient monitoring messages did not lead to any significant number of notification responses from the caregivers. It framed conversations in the evening when the caregiver and user got together. In such situations the caregiver would ask questions in a probing way, even though iSwear did not explicitly report the information, “Why did you have tea twice at the office? I got to know about it from the message…– (CI)”. She asked this question being unsure of what her husband had in the office. iSwear gave her a context informed cue but didn’t give her more factual information. It tuned out the patient-husband had tea just once, and the other sms was a false positive. However, the SMS helped initiate such dialogue exchanges. The caregivers were also not able to make complete sense of the information from iSwear; hence, did not know how to respond to it. One of the caregivers (CI) was excited to receive SMS from iSwear but did not know what it signified or what to do as a follow up. For example, knowing the number of steps her husband had walked confused the caregiver as to whether it was a good practice since this was not on her list of patient monitoring activity. She indicated towards the need of more actionable information from the caregiver’s perspective. She asked, “This is really good. But when should I call him? – (CI)”. This indicated the need for iSwear action prompts instead of showing factual patient information.
Challenges in the Field
In this section, we attempt to elaborate the tensions that ensue when an ethnographer and a designer co-habit in the designing of a care giving system. The designer is more interested in evaluating the system while the ethnographer is loathe to control any in-situ activity to service a design implication. Both authors found a ‘mean’ in balancing and triangulating the study of call logs from iSwear and the personal interviews during the pilot. The three patients identified for the preliminary user study were not facing any kind of acute mobility constraints and were normal in their day-to-day activities. Thus patients would go out of their homes for business-as-usual type of activities other than their morning or evening walk. In one case the user was checked at the entrance of a shopping mall by the security guard because the appearance of iSwear, in his opinion, resembled a bomb-triggering device. The user refrained from wearing the device while going out of his home for the rest of the week. Here, we understand the importance of form and appearance of the device and how an improved and non-intrusive form would have helped the study.
Another important fact to note is that the caregivers were life partners or children of the patient with a long history of domestic co-habitation. This informed their everyday communication practices: phone calls were made during certain times of the day or only on occasions that were deemed as warranting a call. Thus many messages sent during a particular point in time of the day were completely ignored by the caregiver. This also aligns to the fact that caregivers were mostly aware of the context in which the patient was. However, caregivers indicated the need for emergency notifications warranting immediate action.
Evenings were spent in discussing the day’s events especially those that involved health care practices. Families settle into a daily rhythm of communication practices that any system, seeking to mediate health monitoring, needs to take note of and even abstract design principles out of them.
DISCUSSIONS
Any system needs to be designed to take advantage of contextual awareness. Centralizing the role of a caregiver; accounting for the dynamics of role reversals; observing the contextual dynamics in multiple caregiving scenarios are some of the few key implications that can aid in designing for higher acceptance of monitoring systems. The nature and content of communication is of significant importance in such monitoring systems. In this section we discuss some of the open implications from our findings from ethnography and initial feedback from the preliminary field study. These questions and implications can be extended for the design of better CDM communication and wellness persuasion tools.
Accounting for Role Reversals
Our ethnography suggests that wellness and CDM systems should account for unforeseen and situational role reversals. While work of vigilance is important from a caregiver’s perspective, CDM systems should account for its gradual acceptance. This demands higher transparency in wellness monitoring systems and provision for diverse communication protocols, which might also involve auxiliary caregivers for patient monitoring.
Designing Assurance Mechanisms
An important aspect of caregiving is enabling a positive disposition in the patient condition as a result of the caregiving activity. Our ethnographic study suggests that caregivers are in need of regular updating of the patient’s wellbeing and activity. They require perpetual updates about food intake, medicine intake and physical activity, which need to be communicated if the caretaker is remote. A dedicated caregiver not only needs assurance but proof of efficacy for their caregiving activities. This is also a requirement for auxiliary caregivers who can evaluate themselves and receive assurance on their performance. This evaluation can be based on many factors like, monitoring patient progress on their health condition, knowledge about illness and skills in managing different trajectories of work. Caregivers could also collaborate and learn from professional caregivers who can not only augment skills but act as moderator or a caregiving coach. Wellness and CDM systems should tap into the basic needs of caregivers around this sense of assurance and achievement as a skilled person.
Enabling Multiple Persuasion Points
Our ethnographic study showed that even though there is typically one primary caregiver in the family, other members, sometimes neighbors, also play caregiving roles. In-person caregivers and remote caregivers have different contextual awareness. Remote caregivers would face challenges in evaluating patient health or wellness activity adherence. This may lead to a different dynamic of trust between these key actors in a caregiving context.
Similar differences may also occur in terms of closeness in a relationship. An in-person caregiver attracts more trust than a remote one. A caregiver from the family would be closer than a neighbor or a hired help. A more dynamic system could address the need for communicating a diverse set of information to various types of caregivers offering varying degrees of care. Wellness and CDM systems should account for difference in stakeholder roles and patient preferences. Effective and curated communication of information to many kinds of caregivers can make for a powerful persuasion strategy.
Content of Communication
It was observed from our field study that patients expected to be informed about the system status and notifications. Patients felt disconnected from the process of iSwear notifications being sent to their caregivers. Future wellness and CDM systems should engage all stakeholders as active and communicating participants in the system. Another challenge was in the message design. Messages must clearly communicate the present state of the patient, set correct expectations on adherence and wellness activity and inform about coherent intervention required from the caregiver. Information from the monitoring systems should not raise false alarms leading to caregiver panic attacks. Knowledge of CDM and subject matter expertise is another important factor to be considered while designing the content of CDM communications. The reporting or notification systems should be personalized enough to cater to patient centric or caregiver centric needs. A medical report may be useful for an experienced conjugal caregiver but the same may be irrelevant for a remote filial caregiver. Similarly, caregivers may prefer to book-keep patient records or prescriptions, but the same cannot be used as an activity checklist for patients. Expectation of information also varies. We observed caregivers book-keep all records and prescriptions to prepare a simple checklist of activities for self-referencing. While remote caregivers were concerned about the quality of professional care and details of medical adherence, in-person caregivers were involved in the entire inventory management of care. Future wellness and CDM systems should abstract reporting information based on different stakeholder expectations to make it more actionable.
Nature of Communication
Patient monitoring and recommendation for care giving can be targeted to be effective and timely in nature during acute conditions. In the case of chronic conditions, the care required is continuous for long swathes of time. Common physiological parameters that continuously and pervasively monitor the patient can yield a holistic assessment of patient activity even if in varying levels of precision. We realize that the nature of communication in caregiving situations are emotional and affecting rather than technical or to the point. Thus communication between caregivers and patients should be able to represent the emotional quotient while aiming to remove ambiguity about communicating any unusual patient activity.
Future systems should also consider the condition, time of the day and personal preference while sending messages to caregivers. In both the ethnography and the preliminary study, we observed caregivers having extensive discussions with patients once a day. Messages could be tailored around such caregiver preferences. Information specific to infrastructure, work culture and other situational contexts can help in designing time and frequency protocols aimed for the caregiver.
Designing Incremental Interventions
In our preliminary study we observed users struggling to adapt to the iSwear communication protocols. They had difficulty in responding to messages pushed by the device. The device brought in some disruptive triggers to their current caregiving arrangement. Perhaps a week of usage is sub-optimal for the desired adoption but there is definite need for any device or system to be non-intrusive and pervasive enough if it had to remain with the patient all the time. While caregivers wanted systems that could perpetually inform them about the patient’s condition, issues of privacy and the adoption of an always-on technology into a patient’s daily life remain a challenge. A system for CDM should be built to bring in gradual and incremental changes in patient-caregiver routines and lifestyles.
CONCLUSION
Future opportunities for a qualitative and design pilot of iSwear include a more detailed and longitudinal usability evaluation of the iSwear system. We further plan to extend our communication capabilities to a wider stakeholder community such as extended family members and formal caregivers. We discussed some of the open implications on content and nature of communication in a CDM system. These implications can be further extended to design individual persuasion and motivation strategies in a range of wellness monitoring and persuasion applications.
Our ethnography provided an understanding of trust-persuasion quadrants of caregiving. We realize that our ethnography has been serviced to break down ‘trust’ and map them to the presence and nature of relationship between the caregiver and patient- in our case one that resides within Indian families. We would also like to confess our awareness of reducing the caregiving relationship into a function of two discrete variables. We consider this to be a beginning of a discussion about designing systems that are sensitive to and accommodative of complex human motivations and behaviors, no less, in a care giving context. Expanding these quadrants to care work trajectories for specific chronic conditions will offer a deeper understanding of specific care requirements. We hope this will lower the barrier in building caregiver centric applications and engender a new class of wellness and CDM tools. Family ethnographies, designing iSwear, its in-situ pilot capturing caregiver-patient exchanges, post-pilot efficacy mapping, and the evolution of a care ontology to define communication protocols in a care context clearly underline the importance of a data eco-system. Capturing right amounts of patient care feedback data, at critical moments of caregiving helped to comprehend not only a specific care ecosystem but to evolve a generalizable ontological understanding of communication practices in the patient-caregiver everyday repertory.
Jyotirmaya Mahapatra works in the field of Human Computer Interaction. He currently works as Research Engineer with the focus on User Experience Design of various products. He has received his Masters in Design degree in 2012 from Indian Institute of Technology, Bombay (IITB) where he has designed “Graphics management system for high scale visualizations” and “Rehabilitation tools for Tarumatic Brain Injury patients” under the supervision of Prof. Pramod Khambete and Prof. Anirudha Joshi respectively. Prior to joining XRCI he was working as User Experience Designer for Clarice Technologies where he has designed product from various domains such Machine log analytics, Human resources, Database management etc.
Nimmi Rangaswamy is a Senior Researcher at the Xerox Research Centre India, Bangalore. She is a social anthropologist and conducts ethnographic research in the area of work practice and HCI at XRCI. Her research analysis are informed by a variety of social approaches to technology use and thick field descriptions. At XRCI, Nimmi is working on projects in Customer Care and Urban Mobility. Nimmi received her PhD and M-Phil from the Delhi School of Economics and University of Mumbai in Social Anthropology. Nimmi is also currently adjunct professor at the Indian institute of Technology, Hyderabad teaching two courses: “ICT for Development: Debates on Theory and Praxis” and Sociology of Digital Media. Previously, her job at Microsoft Research was a combination of theoretical analysis and ethnographic field research to understand technology use in developing countries. These are studies of patterns of technology adoption in various social contexts and spaces in India, ranging from middle class consumption of domestic media, the business models of cyber cafés and the use of mobile internet and Facebook among urban slum youth.
NOTES
Acknowledgment – The authors would like to thank all the patients and caregivers who participated in the ethnography and the ongoing study of the iSwear system.
1 Here, we use ontology as in the information sciences representing the regenerative knowledge and definition of the types, properties, and interrelationships of the entities that exist for a particular domain of discourse.
REFERENCES CITED
Allen, I., Hogg, D. and Peace, S.
1992 ‘Elderly people in the community: Informal care’, Elderly People: Choice, Participation and Satisfaction, London: Policy Studies Institute at the University of Westminster, pp. 10–38
Andrea Parker, Vasudhara Kantroo, Hee Rin Lee, Miguel Osornio, Mansi Sharma, and Rebecca Grinter.
2012 Health promotion as activism: building community capacity to effect social change. Conference on Human Factors in Computing Systems (CHI ‘12). ACM, New York, NY, USA, 99-108
Aronson JK.
2007 Compliance, Concordance, Adherence. Br J Clin Pharmacol 2007:63:383–4.
Baek Knowl, Duke Kyle, Lou Roy, Lee Monica, and Mathew Anijo
2013 Human API as a research source in health care. Ethnographic Praxis in Industry Conference Proceedings 2013:280–295. https://www.epicpeople.org/human-api-as-a-research-source-in-health-care/
Concolve, S., Roessler, p., Shelton, B.E., LaMarca, A., Schilit, B., and Bly, S.
2004 Technology for care networks of elders. Pervasive Computing, IEEE 3, 2(2004), 22-29.
CSJ (Centre for Social Justice)
2011 Age of Opportunity: Transforming the lives of Older People in the UK. London: CSJ
Donelan K., Hill C. A., Hoffman C., Scoles K., Feldman P. H., Levine C., and Gould D.
2002 Challenged to care: informal caregivers in a changing health system. Health Affairs, 21(4), 222-231.
Duncan, J., Camp, L. J., and Hazelwood, W. R.
2009 The portal monitor: a privacy-enhanced event-driven system for elder care. International Conference on Persuasive Technology, ACM(2009), 36:1-9
Fiore-Silfvast, Brittany and Neff, Gina
2013 What we talk about when we talk data: Valences and the social performance of multiple metrics in digital health. Ethnographic Praxis in Industry Conference Proceedings 2013:89–101. https://www.epicpeople.org/what-we-talk-about-when-we-talk-data-valences-and-the-social-performance-of-multiple-metrics-in-digital-health/
Gandhi, K. and Bowers, H.
2008 Duty and Obligation: The Invisible Glue in Services and Support. York: Joseph Rowntree Foundation
Holman H, Lorig K.
2002 Patients as partners in managing chronic disease. BMJ 2002, 320, pp. 526-527
Jamuna, D.
1997 Stress dimensions among caregivers of the elderly, The Indian journal of Medical Research. Spl.issue: Aging in India, pp.381-387.
John Vines, Gary Pritchard, Peter Wright, Patrick Olivier, and Katie Brittain.
2015 An Age-Old Problem: Examining the Discourses of Ageing in HCI and Strategies for Future Research. ACM Trans. Comput.-Hum. Interact.
Juliet Corbin and Anselm Strauss.
1985 Managing Chronic Illness at Home: Three Lines of Work. Qualitative Sociology, 8(3): 224-247
Kawakita, J.
1991 The original KJ method. Kawakita Res. Inst., Tokyo.
Keating, N., Otfinowski, P., Wenger, C., Fast, J. and Derksen, L.
2003 ‘Understanding the caring capacity of informal networks of frail seniors: A case for care networks’, Ageing and Society, Vol. 23, No. 1, pp. 115–27
Shrivastava, S.R., Shrivastava, P.S., and Ramasamy, J.
2013 Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 12(1):14. doi: 10.1186/2251-6581-12-14.
Slobin Adrian and Cherkasky Todd
2010 Ethnography in the Age of Analytics. Ethnographic Praxis in Industry Conference Proceedings 2010:209–219. https://www.epicpeople.org/ethnography-in-the-age-of-analytics/
Strauss, A., Fagerhaugh, S., Suczek, B, and Weiner, C.
1985 Social Organisation of Medical Work. University of Chicago, Chicago.
Tang, K.P., Hirano, S., Cheng, KG, and Hayes, G.,
2012 Balancing caregiver and clinician needs in a mobile health informatics tool for preterm infants. Pervasive Computing Technologies for Healthcare. (2012), 1-8.
Unrun Kenton T. and Pratt Wanda
2008 The Invisible Work of Being a Patient and Implications for Health Care: “[the doctor is] my business partner in the most important business in my life, staying alive.” Ethnographic Praxis in Industry Conference Proceedings 2008:54–64. https://www.epicpeople.org/the-invisible-work-of-being-a-patient-and-implications-for-health-care-the-doctor-is-my-business-partner-in-the-most-important-business-in-my-life-staying-alive/
Wagner EH, Davis C, Schaefer J, Von Korff M, Austin B.
1999 A survey of leading chronic disease management programs: are they consistent with the literature? Manage Care Q. Summer ;7(3):56-66.
Yunan Chen, Victor Ngo, and Sun Young Park.
2013 Caring for caregivers: designing for integrality. Computer supported cooperative work (CSCW ‘13). ACM, New York, NY, USA, 91-102.
Young, A. F., Russell, A. and Powers, J. R.
2004 ‘The sense of belonging to a neighbourhood: Can it be measured and is it related to health and well being in older women?’, Social Science & Medicine, Vol. 59, Issue 12, pp. 2627–37